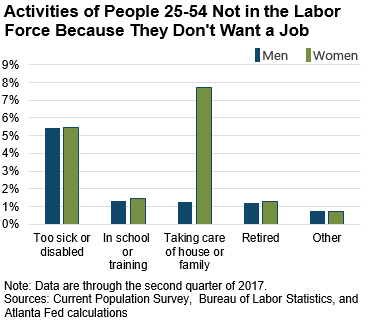
It is well known that poor health is bad for an individual's income, partially because it can lower the propensity to participate in the labor market. In fact, 5.4 percent of prime-age individuals (those 25–54 years old) reported being too sick or disabled to work in the second quarter of 2017. This is the most commonly cited reason prime-age men do not want a job, and for prime-age women, it is the second most often cited reason behind family responsibilities (see the chart). (Throughout this article, I use the measure "not wanting a job because of poor health or disability" as a proxy for serious health problems.)
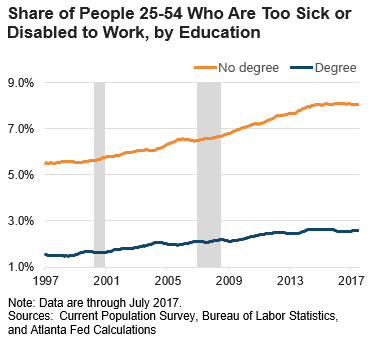
In addition to being prevalent, the share of the prime-age population citing poor health or disability as the main reason for not wanting a job has increased significantly during the past two decades and tends to be higher among those with less education (see the chart).
Yet by some standards, the health of Americans is improving. For example, compared to two decades ago the average American is living two years longer, and the likelihood of dying from cancer or cardiovascular disease has fallen. These specific outcomes, however, may have more to do with improvements in the treatment of chronic disease (and the resulting reduction in mortality rates) than improvements in the incidence of health problems.
Another puzzle—which is perhaps also a clue—is the considerable variation across states in the rates of being too sick or disabled to work. For example, people living in Mississippi, Alabama, Kentucky, or West Virginia in 2016 were more than three times likelier to indicate being too sick or disabled to work than residents of Utah, North Dakota, Iowa, or Minnesota (see the maps below).
This cross-state variation is useful because it allows state-by-state comparisons of the prevalence of specific health problems. Among a list of more than 30 health indicators![]() , the two factors that most correlate with the share of a state's population too sick or disabled to work were high blood pressure (a correlation of 0.86) and diabetes (a correlation of 0.83). Both of these conditions are associated with risk factors
, the two factors that most correlate with the share of a state's population too sick or disabled to work were high blood pressure (a correlation of 0.86) and diabetes (a correlation of 0.83). Both of these conditions are associated with risk factors![]() such as family history, race, inactivity, poor diet, and obesity. Both of these health issues have increased significantly on a national basis in recent years.
such as family history, race, inactivity, poor diet, and obesity. Both of these health issues have increased significantly on a national basis in recent years.

So how might poor health hinder economic growth? Health factors account for a significant part of the decline in labor force participation since at least the late 1990s. After controlling for demographic changes, the share of people too sick or disabled to work is about 1.6 percentage points higher today than it was two decades ago (see the interactive charts on our website). Other things equal, if this trend reversed itself during the next year, it could increase the workforce by up to 4 million people, and add around 2.6 percentage points to gross domestic product (calculated using our Labor Market Sliders).
Of course, such a sudden and large reversal in health is highly unlikely. Nonetheless, significant improvements to the health of the working-age population would help lessen the drag on growth of the labor supply coming from an aging population. Public policy efforts![]() centered on both prevention and treatment of work-impeding health conditions could play an important role in bolstering the nation's workforce.
centered on both prevention and treatment of work-impeding health conditions could play an important role in bolstering the nation's workforce.
 Ellyn Terry, an economic policy analysis specialist in the Atlanta Fed's research department
Ellyn Terry, an economic policy analysis specialist in the Atlanta Fed's research department